Routine shoulder protocols are the most variable, but most include:
Coronal PD FSE
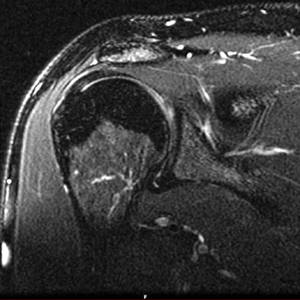
Coronal T2 fat suppressed FSE
Sagittal PD FSE fat suppressed
Sagittal PD FSE
Axial PD fat suppressed FSE

Axial Gradient
Shoulder arthrogram
Coronal oblique rotator cuff imaging
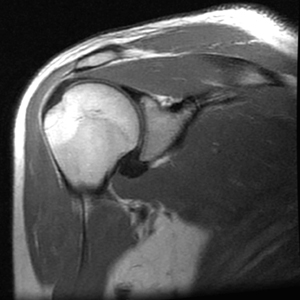
Shoulder Coronal Proton density FSE:
The coronal plane is oblique, paralleling the central tendon of the Supraspinatus muscle. Occasionally, magic angle artifact can cause an increase in signal in the distal Supraspinatus tendon, mimicking a tear or tendonosis
Shoulder Coronal Proton density FSE:
T2 fat suppressed sequencing is used for sensitive detection of abnormal fluid of the distal Supraspinatus tendon. In contrast to an inversion recovery sequence, potential magic angle artifact is eliminated due to the long TE of theT2 sequence.
Magic angle artifact can occur on short TE sequences and can result in tendons/ligaments having erroneous areas of high T2 signal. Normally, transverse magnetization decay is enhanced (and therefore T2 is shortened) in non-random structures such as the parallel fibers of tendons and ligaments. But when tendons/ligaments are oriented at 55 degrees to the magnetic field, magnetization decay is hindered, increasing T2 signal intensity. Longer TE sequences are required to allow for full decay of transverse magnetization/T2 signal.
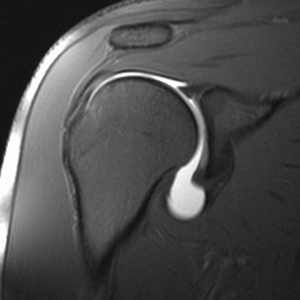
Sagital rotator cuff imaging
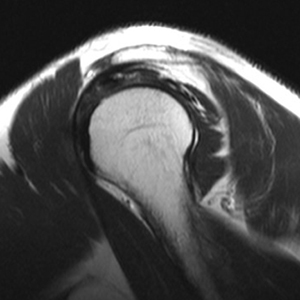
Sagittal Proton density FSE:
The sequence evaluates the acromial arch, including acromial inferior cortex, acromioclavicular joint, and coraco-acromioligament.
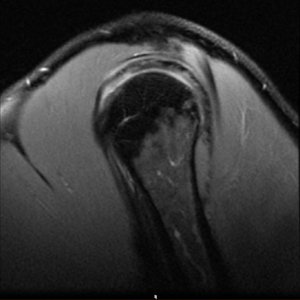
Shoulder Sagittal Proton density, fat suppressed FSE:
This sequence is a 'second look' at the distal rotator cuff tendons. The plane can also be angled obliquely to be more perpendicular to the tendons at insertion.
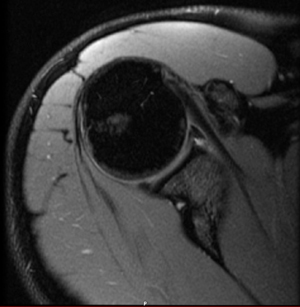
Axial glenoid labrum imaging
Shoulder Axial Proton density, fat suppressed FSE and Axial GRE:
The sequences allow for evaluation of the labrum and glenohumeral ligaments, as well as the glenohumeral cartilage.